Treatment Guidelines
Current guidelines from the American Diabetes Association recommend a person-centered approach to the selection of antidiabetic agents. Key patient factors to take into consideration include: 1) comorbidities, such as atherosclerotic cardiovascular disease (ASCVD), chronic kidney disease (CKD), and heart failure; 2) hypoglycemia risk; 3) effects on body weight; 4) side effects; 5) cost; and 6) patient preferences. Lifestyle modifications that include weight loss, exercise, and healthy diet should be emphasized in addition to pharmacologic therapy.1
Metformin is recommended as first-line therapy for all patients after diagnosis of type 2 diabetes unless contraindicated. Metformin is effective in reducing hemoglobin (Hb)A1C, safe and inexpensive, and has shown benefits in weight and cardiovascular risk. The drug is cleared by renal filtration and should not be used in patients with estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2. Metformin use is associated with vitamin B12 deficiency and worsening of neuropathy symptoms.2 Periodic testing of vitamin B12 is recommended in patients receiving metformin.3 In patients with HbA1c levels >1.5% above glycemic target, dual combination therapy may be required.1
The early introduction of insulin should be considered if there is evidence of ongoing catabolism (weight loss), if symptoms of hyperglycemia are present, or when A1C levels (>10% [86 mmol/mol]) or blood glucose levels (≥300 mg/dL [16.7 mmol/L]) are very high.As glucose toxicity resolves, simplifying the regimen or changing to oral agents may be possible.1.
If the A1C target is not achieved after approximately 3 months, metformin can be combined with any one of the preferred six treatment options: sulfonylurea, thiazolidinedione, DPP-4 inhibitor, SGLT2 inhibitor, GLP-1 RA, or basal insulin; the choice of which agent to add is based on drug-specific effects and patient factors. Considerations include cardiovascular comorbidities, hypoglycemia risk, impact on weight, cost, risk for side effects, and patient preferences. For patients with established ASCVD or indicators of high ASCVD risk (such as patients ≥55 years of age with coronary, carotid, or lower-extremity artery stenosis >50% or left ventricular hypertrophy), established kidney disease, or heart failure, an SGLT-2 inhibitor or GLP-1 RA with demonstrated CVD benefit is recommended as part of the glucose-lowering regimen independent of A1C and in consideration of patient-specific factors. For patients without established ASCVD, indicators of high ASCVD risk, HF, or CKD, the choice of a second agent to add to metformin is not yet guided by empiric evidence. Rather, drug choice is based on avoidance of side effects, particularly hypoglycemia and weight gain, cost, and patient preferences. Similar considerations are applied in patients who require a third agent to achieve glycemic goals. In all cases, treatment regimens need to be continuously reviewed for efficacy, side effects, and patient burden.1
Patients may eventually require injectable medications to reach their glycemic target as these agents have higher potency. Basal insulin or GLP-1 receptor agonists may be used in patients not meeting glycemic goals with oral agents. Trials comparing GLP-1 receptor agonists to insulin as add-on therapy found similar efficacy with both agents. However, GLP-1 receptor agonists decrease body weight and have a lower risk of hypoglycemia than insulin. Although GLP-1 receptor agonists are more likely to cause gastrointestinal side effects, they are the preferred option in patients requiring the potency of injectable agents for glucose control.4,5,6
If basal insulin has been titrated to an acceptable fasting blood glucose level and HbA1c remains above target, a combination injectable product containing basal insulin and a GLP-1 receptor agonist may be considered. This combination is effective in lowering HbA1c and produces less weight gain and hypoglycemia compared to intensified insulin regimens. If a combination injectable product is used, metformin should be continued while sulfonylureas and DPP-4 inhibitors should be discontinued. Some patients with suboptimal blood glucose control may require adjunctive thiazolidinedione or SGLT2 inhibitor therapy. Two different once-daily fixed-dose combination products containing basal insulin plus a GLP-1 receptor agonist are available: insulin degludec plus liraglutide and insulin glargine plus lixisenatide.7,8,9
Figure 1: Guideline Recommendations for the Pharmacologic Management of Type 2 Diabetes1
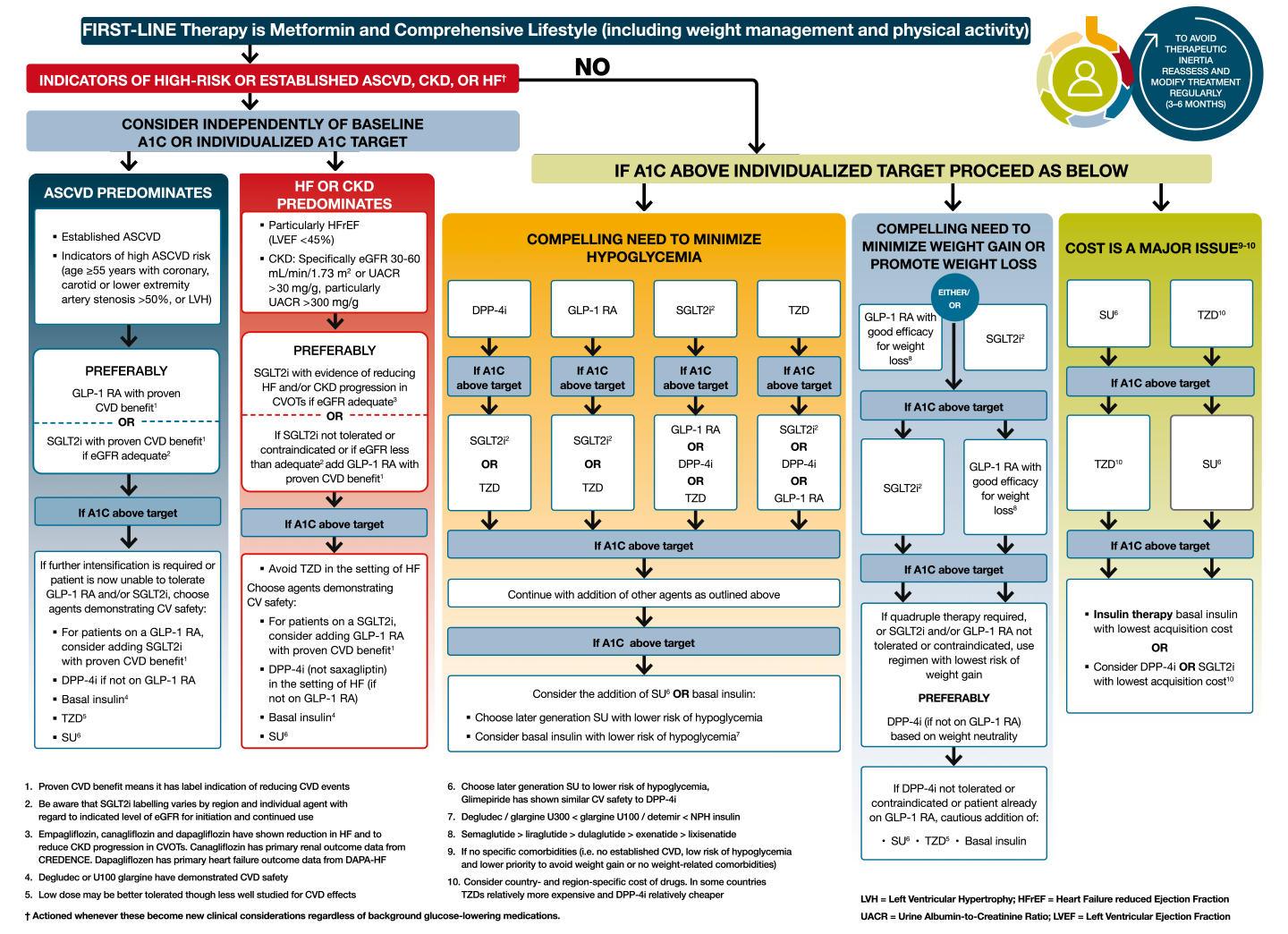
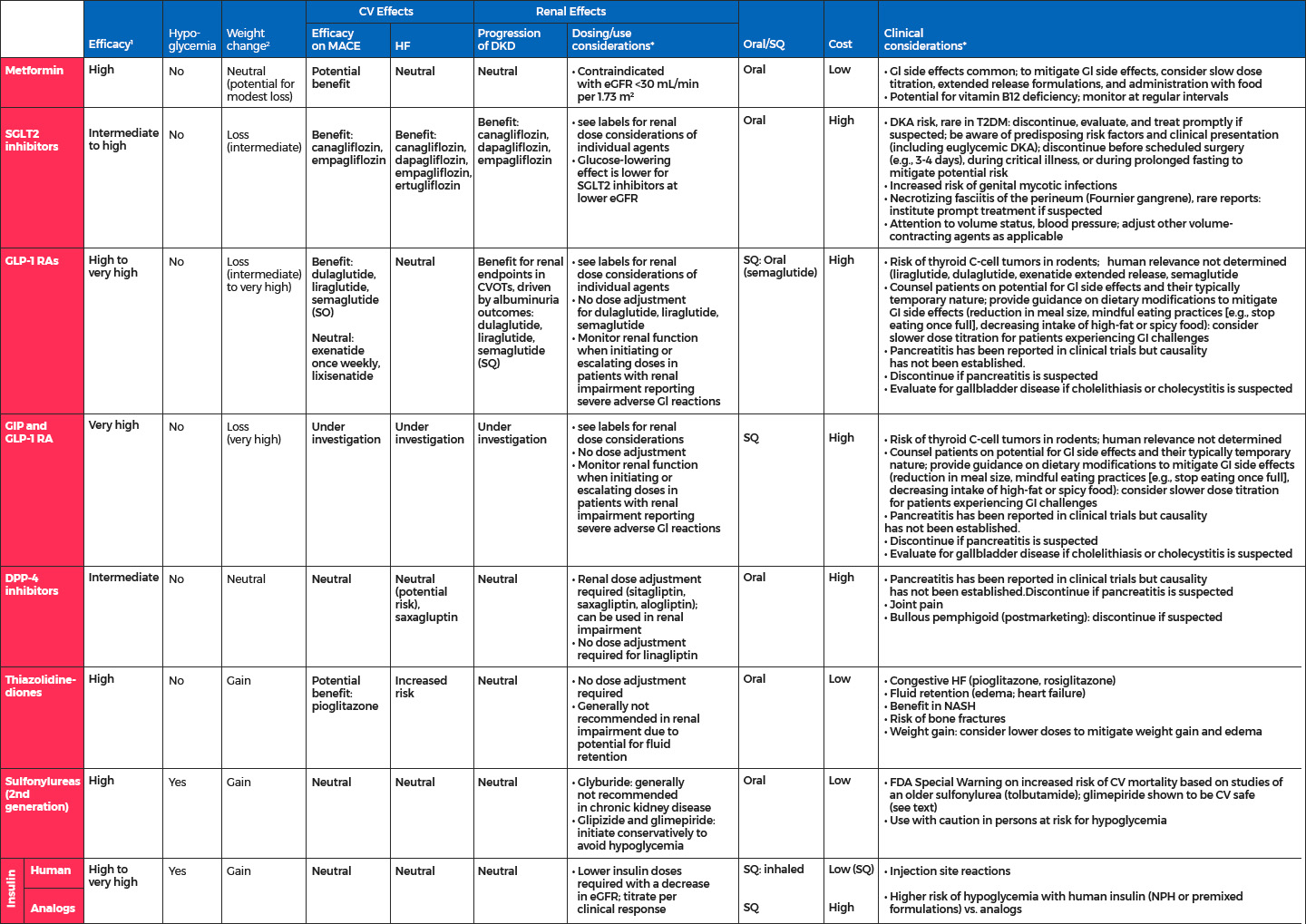
Figure 2: Summary of Medications for Lowering Glucose1
References
- American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of medical care in diabetes—2023. Diabetes Care. 2023;46(suppl 1):S140-S157.
- Out M, Kooy A, Lehert P, et al. Long-term treatment with metformin in type 2 diabetes and methylmalonic acid: Post hoc analysis of a randomized controlled 4.3 year trial. J Diabetes Complications. 2018;32:171-178.
- Aroda VR, Edelstein SL, Goldberg RB, et al. Diabetes Prevention Program Research Group. Long-term metformin use and vitamin B12 deficiency in the Diabetes Prevention Program Outcomes Study. J Clin Endocrinol Metab. 2016;101:1754-1761.
- Singh S, Wright EE Jr, Kwan AYM, et al. Glucagon-like peptide-1 receptor agonists compared with basal insulins for the treatment of type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Obes Metab. 2017;19:228-238.
- Levin PA, Nguyen H, Wittbrodt ET, et al. Glucagon-like peptide-1 receptor agonists: A systematic review of comparative effectiveness research. Diabetes Metab Syndr Obes. 2017;10:123-139.
- Abd El Aziz MS, Kahle M, Meier JJ, et al. A meta-analysis comparing clinical effects of short- or long-acting GLP-1 receptor agonists versus insulin treatment from head-to-head studies in type 2 diabetic patients. Diabetes Obes Metab. 2017;19:216-227.
- Diamant M, Nauck MA, Shaginian R, et al. 4B Study Group. Glucagon-like peptide 1 receptor agonist or bolus insulin with optimized basal insulin in type 2 diabetes. Diabetes Care. 2014;37:2763-2773.
- Eng C, Kramer CK, Zinman B, et al. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: A systematic review and meta-analysis. Lancet. 2014;384:2228-2234.
- Maiorino MI, Chiodini P, Bellastella G, et al. Insulin and glucagon-like peptide 1 receptor agonist combination therapy in type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Care. 2017;40:614-624.